CTA and Stress Tests for Chest Pain Lead to Similar Clinical Outcomes
| Figure 1. PROMISE results suggest that both the CTA and functional stress-test study groups experienced similar rates of heart attack or other serious event during the 2-year study follow-up period | 
|
|
| Figure 2. PROMISE results suggest that CTA may offer the benefit of fewer unneeded invasive catheterizations. Only 3.4% of those in the CTA group compared with 4.3% of the stress-test group underwent the unneeded procedure | 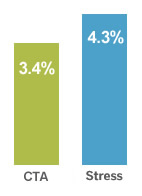
|
In the first head-to-head comparison of the clinical effectiveness of diagnostic tests for coronary artery disease, the relatively new technique of coronary computed tomographic angiography (CTA) was shown to perform as well as traditional stress tests in terms of future, major cardiac events. The new CTA technique also resulted in fewer unneeded catheterizations and less radiation exposure.
Dubbed the PROMISE trial, the study involved 10,003 patients at 193 centers across the United States and Canada. Study participants with symptoms such as chest pain were randomly assigned to receive either CTA or a functional stress test to evaluate the possibility of coronary artery disease. The particular stress test each participant received—exercise electrocardiogram, stress nuclear imaging, or stress echocardiogram—was selected by the team caring for the patient and was consistent with “standard of care” of the practice setting.
Both CTA and stress tests resulted in low rates of serious outcomes; 3.3% of those who underwent CTA and 3.0% of those who underwent functional stress test experienced heart attack or another serious event during the 2-year follow-up period (Figure 1).
The results could be the first step toward greater acceptance and insurance coverage of CTAs for chest pain, according to lead study author, Pamela Douglas, MD, Geller professor of research in cardiovascular diseases at the Duke Clinical Research Institute. “The outcomes are excellent and similar regardless of which kind of diagnostic test you use. Patients should work with their doctors to determine the best test for them,” Douglas advises.
Douglas says that the researchers undertook the study because “the question has been whether CTA has the potential to reduce unnecessary invasive testing and improve outcomes because it is substantially more accurate in detecting important obstructive and nonobstructive coronary artery disease.”
She notes that the researchers were pleasantly surprised at the low rate of serious cardiac events in both sets of participants and that the number of events was so low in the stress-test participants that it would be difficult for a new test to improve on it. Compared with functional testing, CTA did not reduce the incidence of heart attacks, hospitalizations for unstable angina, major procedural complications, or death during a median of 25 months of follow-up, but it did seem to offer advantages in guiding follow-up testing.
Those who received CTA had fewer unneeded invasive catheterizations: just 3.4% of the CTA group had catheterizations that showed they were free of disease compared with 4.3% of the stress-test group (Figure 2). Radiation exposure was also lower for those in the CTA group than it was in those receiving nuclear tests.
A current drawback of CTA is that few insurers pay for it as a diagnostic test for suspected coronary artery disease related to chest pain, but the potential advantages in some situations suggested in this study could lead to greater acceptance.
“PROMISE establishes CTA as a viable alternative to stress testing for the evaluation of patients with suspected coronary disease,” says Udo Hoffman, MD, principal investigator of the PROMISE Imaging Core and director of cardiovascular imaging at Massachusetts General Hospital.
“Our study provides a real-world assessment of how testing in patients with chest pain has an impact on their subsequent health. We had very little high-quality evidence to guide decision making for how to evaluate these patients,” Douglas says. “The message for clinicians is that the outcomes are excellent and similar regardless of which kind of diagnostic test you use.”
Because CTA is a scan that uses fast imaging with intravenous dye to show blockages of the coronary arteries, it could become the test of choice when a clinician wants to view the structures around the heart.
The trial was funded by the National Heart, Lung, and Blood Institute. Results were presented at the March 2015 American College of Cardiology meeting and published online in the March 14, 2015, New England Journal of Medicine.