Making Aneurysm Repair Safer and Faster
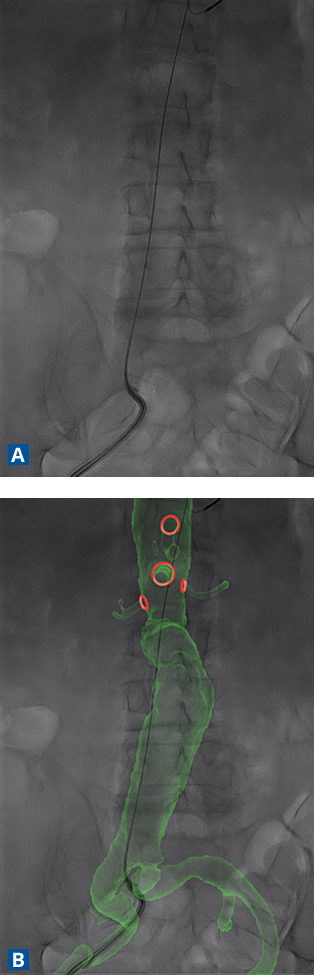
FIGURE A–B. (A) X-ray without imaging technology. (B) X-ray with imaging technology overlay. Images courtesy of Cydar EV.
Duke vascular surgeons have begun using a pioneering 3-dimensional (3-D) imaging technology that provides real-time, enhanced visual map guiding endovascular aneurysm repair (EVAR).
Since May, the Duke vascular team has performed more than 50 procedures using fully automated 3-D imaging system developed by Cydar EV (Cambridge, UK). The software generates crisp digital images while seamlessly integrating fixed and mobile X-ray systems (Figure).
Duke University Hospital is the only medical center in the United States using the technology.
Cynthia K. Shortell, MD, chief of vascular and endovascular surgery and acting chief for trauma and critical care surgery, introduced the technology to Duke after training with Cydar EV, the UK-based creator and manufacturer.
“It has been an instant, blockbuster hit with everyone involved in these procedures,” Shortell says. “Every operating room participant has a story about the way this technology benefits our team—shorter procedures, lower radiation, less contrast agent, and much greater accuracy.”
The improved images have resulted in several advantages:
- Reduction in use of contrast agent volume by 38%
- Reduction in X-ray screening time of 43 minutes per procedure (approximately 35%)
- Reduction in average total procedure time of 53 minutes
Previously, Duke surgeons studied preoperative 3-D images captured by computed tomography (CT) before surgery. During the procedure, they used 2-dimensional (2-D) images as part of the X-ray intervention to place the stent graft within the aorta. Images would register to the patient’s position; when the patient moved, surgeons had to wait for the image to register again. Visual accuracy was limited to a range of 7 to 8 milliliters. Procedures required slow, deliberate steps. The fusion-imaging technology, which allows physicians to follow the patient seamlessly, provides a much more precise level of visual accuracy.
“One of the challenges we face when doing complex EVAR is working with a 2-D image we see on fluoroscopy screen,” Shortell says. “But, obviously, we are working within a 3-D structure—the aorta—and we are moving wires through branches and trying to position the graft.”
The real-time imaging optimizes surgeons’ ability to access vessels and reduces total operative time, which in turn reduces radiation exposure to patients and staff members.
In traditional EVAR procedures, the contrast agent is the leading cause of hospital-induced kidney insufficiency. “By using less, we can avoid tipping the patient into dialysis after the procedure,” Shortell says.
The cloud-based technology synchronizes with existing imaging systems within the hospital, Shortell says, and can be incorporated into operating suites without expensive upgrades.
Some benefits to patients are preventive in nature and subtle—requiring less anesthesia, for example, and reducing radiation burns.
“But, overall, our outcomes are better,” Shortell says. “Shorter stays in the hospital, fewer kidney problems, and simpler, more accurate procedures.”
The company name—Cydar—is an acronym for a question asked frequently in operating suites while the technology was being developed: “Can you do another registration?” The technology was developed in a partnership between imaging experts and experienced EVAR surgeons.